
Illustration by Luis Mazon
Kevin Patterson is a specialist in internal medicine and author whose books include News from the Red Desert and Outside the Wire: The War in Afghanistan in the Words of Its Participants.
Ted Barris is an award-winning journalist, broadcaster and author whose books include Dam Busters: Canadian Airmen and the Secret Raid Against Nazi Germany and, most recently, Rush to Danger: Medics in the Line of Fire.
They held their discussion over e-mail in October and November.
Ted Barris:
In the course of writing Rush to Danger, I reflected on the media and pop-culture mythology to which I was exposed as an adolescent in the 1950s and ’60s. I grew up watching war-movie classics and, as a university student, watched the sitcom M*A*S*H, about medical teams in the Korean War. But I’ve always found myself driven to read more, dig deeper, search further for the real figures that might have motivated the creators to build such iconic wartime characters. And they’re there.
As an example, I was struck by the doctor Major Clipton, played by James Donald, in The Bridge on the River Kwai. In the movie, Clipton does his best to keep malnourished, disease-ridden and injured POWs alive, while Colonel Nicholson, played by Alec Guinness, seems bent on building the Japanese commandant’s railway bridge, no matter how many of his fellow POWs it takes.
In fact, the real doctor saving lives in the face of the Japanese using Allied prisoners as forced labour on the Siam-to-Burma railway was a Canadian: Dr. Jacob Markowitz. And Dr. Markowitz’s experimental medicine – using exclusively makeshift utensils and jungle remedies – ends up being even more fantastic than any Hollywood screenwriter’s imagination. He performed 3,800 transfusions, 7,000 procedures and probably saved more than 5,000 men from certain death during the railway’s murderous construction in the Second World War.
Truth is stranger than fiction.
Kevin Patterson:
I agree, it is surprising how rarely military medics have been depicted in detail in literature and in film.
In the 18 years of war that have followed 9/11, we have seen many treatments of snipers, for instance – American Sniper was the highest grossing film in 2014. But that role – killing from a distance – is so much less heroic. Medics are more exposed to danger, and their role, treating both friendly and injured combatants, is more complicated and nuanced.
Is it because filmmakers and writers are preoccupied with the narrative power of death-dealing? A close examination of the medic’s role will necessarily depict the horror of war, and perhaps filmmakers are uncomfortable with that. But one would think that less bellicose artists would find this a natural and fascinating topic.
A brief excerpt from the HBO miniseries Band of Brothers shows medic Eugene Roe, played by Shane Taylor, treating a wounded comrade.
Barris:
Odd coincidence that you mentioned 9/11. Just two days before the terrorist attack, HBO aired the first episode of Band of Brothers. Keenly aware of Stephen Ambrose’s original book and Steven Spielberg’s series adaptation, I tuned in to Episode 6, “Bastogne,” to see how the series portrayed U.S. Airborne medic Eugene Roe. My father, Alex Barris, served with the 319th Medical Battalion in George Patton’s U.S. Third Army fighting under similarly bitter conditions in the Battle of the Bulge, as the Allies pushed the Germans back through the Ardennes and past the former Siegfried Line inside Germany.
The episode accurately showed actor Shane Taylor (as medic Roe) nearly freezing to death, with no winter clothing or lined boots for himself or his fellow medics, and worse, meagre medical supplies for his wounded – scrounging for dressing packs, scissors, drugs and even keeping syrettes of morphine from freezing by wedging them in his armpits. More than any other depiction of army medics, I related to that one. It was my father’s story in frigid technicolour dealing with what he called “mass cals” (massive casualties) and little to treat them with but common-sense medicine.
Patterson:
I think you’re on to something important when you emphasize how Band of Brothers and some other depictions forefront the essential and defining aspect of war – suffering.
The cinematography in the opening minutes of Saving Private Ryan – also made before 9/11 – shocked viewers with its muted colours and its frank unsparing examination of agony. Giovanni Ribisi’s character, medic Wade, was one of that film’s principal characters. Medics are the first and most intimate observers of the worst thing humans do to one another, and any narrative lens that is interested in the horror of war will tend to dwell on their point of view.
Other films that gave prominent roles to medics included 2001′s Black Hawk Down and We Were Soldiers, which was released in 2002, but written before 9/11. It seems to me that depictions of war made after 9/11, especially in the first years of the war, were more likely to be drawn to ideas of righteous revenge.
Here, we’ve mostly been discussing films, though. Are there novels and non-fiction works you can recommend to readers interested in the complex role of military medics? What secondary sources moved you, as you were preparing to write your book?
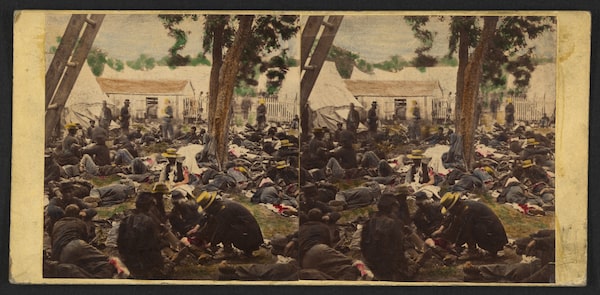
A hand-coloured stereo card shows wounded Union soldiers being tended to at Savage's Station in Virginia during 1862's Peninsula campaign of the U.S. Civil War.James Gibson/The Library of Congress
Barris:
Probably because military medicine experienced such radical change, but also because medics, nurses and others wrote down what they saw on or near battlefields so vividly at Bull Run, Fredericksburg and Gettysburg, journals from the U.S. Civil War proved among the most striking to me.
Once read, I can’t ever erase such views of carnage as that of former journalist, and later army commander, Carl Schurz. He noted in his Reminiscences (1863) “stretchers coming in dreadful procession” and surgeons with rolled up sleeves, blood-stained aprons and “knives not seldom held between their teeth” and the “beseeching eyes of the dying boy who recognized me, says with broken voice, ‘Oh, General! Can you not do something for me?’ And I can do nothing but stroke his hands and utter some words of courage and hope, which I do not believe myself.”
But on the other hand I was attracted to the memoirs of Jonathan Letterman, the Pennsylvania doctor-turned-medical-officer who drags the army brass kicking and screaming into officially accepting field ambulances, real surgeons (not quacks), hygiene, and behind the lines, hospitals with stewards, nurses and cooks to attend the wounded. Some called him a “medical dictator” for his unflinching directives to Union Army strategists who demanded ammo over ambulances, but as the Army of the Potomac’s chief medical officer, Letterman is credited with changing “a vast sea of misery” into medical treatment of wounded “at least equal to the best of the fighting men in gallantry.” His impact on military medicine was the 19th-century equivalent of penicillin, or the Black Hawk medivac helicopter in Iraq and Afghanistan.
Patterson:
Your mention of helicopter evacuation for combat casualties is interesting. This has made a dramatic difference in survival rates in the combat injured. This began in Vietnam, but the technique was more fully developed in the Iraq and Afghanistan wars.
Medics played a very important role, too, in the recent improvements in outcomes by providing early stabilization and resuscitation, including even surgical procedures on the battlefield such as chest tube placement and tracheostomies prior to evacuation. I saw this done regularly in Afghanistan, but I’ve never seen such techniques delegated to non-physicians in the civilian sphere. The stereotype of military culture is that it is intensely hierarchical and conservative, but in this instance it seems less so than civilian medical culture, where physicians keep these skill sets largely to themselves.
More broadly, the position of the medic/medical assistant/corpsman doesn’t really have an analogue at all in civilian life. Physician assistants and EMTs in civilian life do not operate with the same autonomy as their military counterparts. Part of this is pure pragmatism – the volume of trauma seen in war dwarfs that in civilian life.
But I wonder if there may be inspiration to be found in the military experience for making health-care hierarchies more horizontal in the broader world. Are you aware of medics who have advocated for this, upon leaving the military? Did you find that medics often remained in health care after finishing their service?
In Afghanistan, U.S. Army soldiers carry a comrade wounded by an improvised explosive device to a Blackhawk Medevac helicopter in 2012.Shamil Zhumatov/Reuters
Barris:
Your point about helicopter evacuation and its impact on survival rates among combat casualties is a vital one.
Somewhere in my research about medical practice during the Korean War, I unearthed statistics to support your thesis. Mortality rates during the Korean War were 34 per 1,000 wounded; it had been 66 per 1,000 in the Second World War. That statisticians went on to say that a wounded soldier in Korea benefited from greater accessibility to air-evacuation transportation, the advent of better medication – especially antibiotics – and quicker access to surgical and emergency treatment.
Those advancements on the battlefield are borne out in an interview I conducted with Dan Harden, a United States Air Force veteran of military deployments to to Bosnia, Kosovo, Iraq and Afghanistan. During 122 different medieval missions overseas, Major Harden’s emergency ward was the back of a Black Hawk helicopter, where both he and his wounded patient were harnessed into position; and as Harden attended his wounded with oxygen, suction, ventilation, intubation, intravenous or transfusion, the chopper was flying at 140 miles an hour across the desert to deliver Harden’s patient to a contingency operating base for life-saving surgery. Harden told me, “If a wounded soldier was alive after injury, and a medic arrived in that critical time, a patient had a 97-per-cent chance of survival.”
I can think of field ambulance medics at Ypres losing up to 5,000 in the German chlorine-gas attacks of April 1915, or the medical officers in Japanese POW compounds along the so-called Death Railway in the jungles of Burma where up to 4,000 POWs died of disease, injury or exhaustion, or the 916 Canadians that Royal Canadian Army Medical Corps medics could not save on the beaches of Dieppe in August, 1942. Those medics would have sacrificed everything to be able to enjoy a 97-per-cent survival rate among their wounded. But small-box ventilators (gas masks), anti-bacterial drugs and medevac choppers weren’t around to deliver such miracles then.
Patterson:
These successes in improving the survival rates among the (Western and allied) war wounded are probably underappreciated. And the refinements in trauma care in war have spread to the civilian sector, not just in the most recent wars, but for a century now.
Nevertheless, to describe the effect of war, especially on health, in any sort of positive sense is uncomfortable. The excess mortality – including knock-on effects – in Iraq following the invasion may have been almost seven hundred thousand, according to the British medical journal The Lancet. These wars have been the worst decision the West has made in the past half-century.
That said, military medics are in an interesting position. When I was a medical officer, we were taught that our role was to preserve the operational capability of the military. Simply put, soldiers are more likely to fight aggressively if they see that they will be cared for, once wounded.

On an English beach in July, 1942, the Royal Canadian Army Medical Corps rehearses treating 'casualties' ahead of Operation Jubilee, the raid on Dieppe.Department of National Defence / Library and Archives Canada
Barris:
I have one last thought on the point about medics and their service being underappreciated. I think even the medics themselves felt inadequate. More often than not, they took the casualty rates extremely hard. With seemingly very little positive in the aftermath of a battle, medics grasped at whatever small victories they could rationalize.
Two such medical officers – Laurence Alexander with the Calgary Tanks, and Wesley Clare with Royal Hamilton Light Infantry – went into beaches of Dieppe on Aug. 19, 1942 – of 4,963 Canadians in action at Dieppe, 3,367 were killed, wounded or taken prisoner.
Neither Alexander nor Clare managed to get off the beach. In fact, Alexander never left the tank landing craft bringing his medical crew and tank crews ashore; he spent the entire morning dashing from one wounded case to another all aboard the landing craft. And in the end, of his original assault group of 117 military men and 13 naval men, he managed to save but 30 soldiers and three navy personnel.
Meanwhile, Clare gathered the wounded and dying RHLI troops in the lee of another bombed out landing craft just up from the surf. He’d been unable to save 197 of his regimental brothers, but chose to surrender the remaining handful, including himself, to ensure that at least a few survived the slaughter. He spent the rest of the war with those he’d saved in German POW camps in occupied Europe.
And the Calgary Tankers whom Alexander saved never forgot him, either. When Doc Alexander returned to Alberta after the war, the veterans who returned with him made it their business to seek the doctor out to deliver their children and be their family doctor. Small but meaningful thanks for saving them from the “nine bloodiest hours in Canadian military history” at Dieppe.
For further discussion: More from Globe Opinion
What does it mean to be homeless as an Indigenous person? Jesse Thistle and Helen Knott
How does one overcome grief? Julia Samuel and Cathy Rentzenbrink
What is forgiveness? Carys Cragg and Ramin Jahanbegloo
Should women be angry? Rebecca Traister and Soraya Chemaly
What is a mother? Jessica Friedmann and Meaghan O’Connell
Keep your Opinions sharp and informed. Get the Opinion newsletter. Sign up today.